


02 May A Ventilator Making Adventure in Quarantine Days
Open, Close, Measure
Year 2007, working as a freelancer in Istanbul, I am designing an electronic control board for the automatic inflation of car tires with nitrogen gas for a company based in Ankara.
With a 10-bar oil compressor and a spare tire that I brought to my small house’s garden in Hisarustu , the control board and the algorithm that came out after 2 years of work is able to inflate -whether a truck or bicycle- any size of tire (unlike the Australian origin automatic tire inflation device which is also the distributed by the company) quickly and safely.
Tire inflator contol board that I made in 2007

This is achieved by estimating the time to the target pressure by calculating a kind of elastic resistance of the tire to be inflated and automatically adjusting the required PID coefficients -thanks to the control lessons I received from Prof. Kadri Özçaldıran-. With tiny iterations… open valve, close valve, measure the pressure…
At the end of this project, in which — at that time- I thought I didn’t get what I deserved, a patented device which is still exported emerges. By signing an agreement indicating that I will not work for 10 years on a similar subject, I’m delivering all hardware and software files.
Breathe In, Breathe Out, Wait.
March 24, 2020. The BBC reports the following news. In Italy, the 72-year-old priest Giuseppe Berardelli passed away after giving away to a young man the respiratory device that town-people bought for himself . My relatives come to my mind. Is there a sufficient number of ventilator in Turkey? Can these ventilators be reached in a possible emergency? What is a ventilator, how hard can it be? How is it different from inflating a tire? I can not sleep .. Breathe in , breathe out, think..
As a result of my first search; I learn that a ventilator with all functions is quite complicated and the price starts from 10 thousand dollars. Can’t a ventilator consisting of everyday parts that serve a certain purpose be made? I’ll start if I can define the question. After a few weeks I find my question: What should be the leanest ventilator?
Ventilator Problem (What should be the simplest ventilator?)
Imagine a ventilator;
Which is simple to make. Which has no parts made of 3D printers. Consists of standard parts with proven sustainability and reliability. That can be produced in a short time. Which has no unnecessary parts and functions. Minimum number of people and a minimum level of knowledge is sufficient to operate. Easy to manufacture. Which doesn’t allow misuse. And of course meets all medical emergency ventilator requirement (https://www.gov.uk/government/publications/coronavirus-covid-19-ventilator-supply-specification/rapidly-manufactured-ventilator-system-specification).
Open source or not, there are at least 4 values that need to be set even in the most basic ventilators. And a commercial ventilator consists of an average of 100–200 pieces.
The ventilator in my mind —and still has not changed — is a button-free device that recognizes the patient’s liver. It is a 20–30 standard mechanical part that can auto-adjust the pressure and volume values, breathing rate, breathing period and oxygen percentage. Or at maximum with one or two buttons to select the phase of the disease and the operating mode according to the patient’s condition.
More than 100 Ventilator Projects are Emerging with Covid-19
Due to the need for a ventilator after the Covid-19 outbreak (which I have read in some African countries, there are just 2–3 ventilators), more than 100 projects are emerging in the world, most of which are open source.
The ventilator produced by NASA below has one of the simplest interface as far as we can see.
Covid-19 Ventilator, published by Nasa on April 23, 2020

90 percent of open source projects are about squeezing plastic-artificial-respiration-volumes called BVM (Bag Valve Mask) or Ambu set. Ambu set provides a ready-made mechanical working environment with valves, hoses and receptacles on it. However, most healthcare professionals believe that for Covid-19 cases, it will do more harm than good, as it does not meet the required control criterias.
BVM (Bag Valve Mask) based Ventilator developed at Rice University

More than 100 open source ventilator projects can be accessed from the link below.
https://docs.google.com/spreadsheets/d/1inYw5H4RiL0AC_J9vPWzJxXCdlkMLPBRdPgEVKF8DZw/edit#gid=0
When we examine the projects in detail, we can see that only 1 to 2 can approach the level of intensive care unit standards.
However, the fact that many people strive for a solution does not mean that the problem is solved.
In addition, there are big companies that have the mission of producing ventilators with government support in almost every country. Since large companies work with their stakeholders and stakeholders work with smaller companies specialized in their field, complex and hard-to-reach devices that cost $5–10 thousand at the end of the supply and production chain are likely to emerge.
As one of the most successful examples in the world, we can demonstrate Turkey’s bringing together a small ventilator venture with private and public institutions (not profiting in this project) and achieving mass production of multifunctional , high-tech ventilators in less than a month.
In Turkey, ventilators produced jointly with Arçelik, Baykar, Biosys and Aselsan engineers

Some of the ventilators -that are planned to be manufactured 5000 unites at the end of May-, are being donated and exported to other countries, since Turkey does not need at the moment.
Returning to our lean ventilator problem;
A small curious boat can change direction faster and discover more things than the large ships.
So it is a necessary to think small… and sometimes very small.
First Experiments
I have almost everything at home, including an oxygen concentrator. Various microprocessors I’ve been using for years, all Raspberry Pi , arduino modules, pneumatic fittings, valves, pipes, a 12 years-old compressor, and two low pressure sensors (MPXV5010DP and MPVX7002DP) left from an -luckily- uncompleted project. I should mention that those sensors are the only “accessible” sensors in this country and around the world to measure airway pressure and flow.
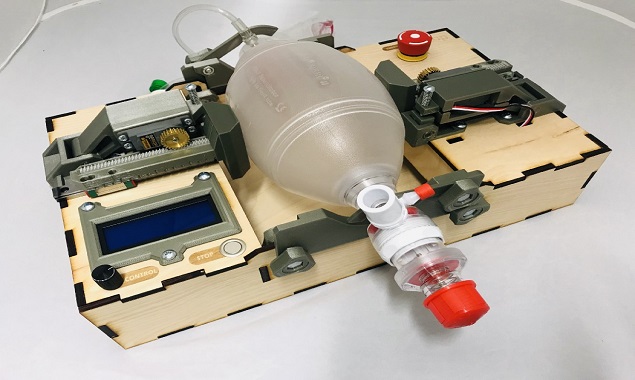
My first prototype:
A prototype I made to test the direct- solenoid valves in my hand, while not aware of how important test-lungs are.
For a realistic test, lung resistance (friction of air) and compliance (volume change against unit pressure change) must be at known values. So in my next experiments, I use the glass for test-lungs, especially after reading the following article.
My Glass Lung — Compliance / Resistance C10 / R5

But is the mechanical ventilation so simple?
Mechanical Ventilation
First of all, underlining that I am not a doctor, will try to summarize ventilation with a paragraph:
The diaphragm muscle contracts and relaxes with the signals from the spinal onion, creating a pressure difference within the lungs. In cases where oxygen-carbon dioxide exchange which occurs between 400 million alveoli and the capillaries is insufficient (which is called Acute Respiratory Distress Syndrome), patients (usually calmed with medication) are connected to the ventilator and continue their vital activities.
The aim of the ventilator is to keep the oxygen pressure in the blood and the rate of inhaled oxygen (PaO2 / FiO2) at certain levels.
The pressure-volume mathematical model of the passive breathing system is formulated as follows.
Pressure (t) = Volume (t) / Compliance + Resistance x Flow (t)
Depending on the value you fix in the ventilators, it is defined as pressure controlled ventilation (PCV) or volume controlled (VCV) ventilation.
There are also functional main modes of operation such as ACV (Assist Control Ventilation), SIMV (Synchronous intermittent mandatory ventilation). An important feature is the ventilator’s detecting natural breathing and synchronizing with the patient.
There are many parts of a ventilator- even it is a very lean one- that needs to be tested and requires help and time. With a post that my wife came across on twitter, the probability of being part of a whole outweighs to combine these pieces.
My participating in CSSALT Ventilator Working Group
A paragraph my wife came across on Twitter is about Florifa University’s open call for support for the emergency ventilator. Requirement documents are clear and simple. My membership is being accepted within a week. This is a group where doctors and mostly amateur radio professionals come together. And it is carried out by CSSALT (University of Florida Center for Safety, Simulation, and Advanced Learning Technologies), with an aim of making an accessible, FDA approved ventilator,
My goal is to catch up on developments and to see how much I can help with my sensor, microprocessor and pneumatic experience.
Scheme of the ventilator device targeted by the working group:
Design scheme of the CSSALT group for the targeted ventilator system

You can find all the requirement documents of the ventilator here.
Open-Source Ventilator Project
Basic Ventilator Problems and Some Solutions in the CSSALT Working Group:
The working group, led by anesthesiologist and amateur radio professional Gordon Gibby, has made progress on most of the issues. Hoses from PVC pipe, arduino microprocessor, sensor selections, flow meter, high pressure protection and anti-drowning valves seem okay.
PVC pipes provide a solid foundation for inlet and outlet ports and are compatible with standard 22mm diameter breathing circuits in commercial ventilators.
In the first version of CSSALT, exhalation control is achieved with passive bicycle rubber

The 3 main problems discussed and solutions found in the group are:
1-Low resistance exhalation solenoid valve problem:
One of the major problems is to find a low airway resistant valve on the exhalation side. Direct solenoid valves with diameters of 20mm and above are quite expensive.
The solution offered by Marc Alan in the group, the photo of which you see below; Rainbird garden watering valve is modified and the valve is turned into a remote pilot valve by controlling it with air pressure instead of electric solenoid. This results in a low resistance valve with no back pressure. 2 million on-off tests ,in the group ,made by Bob Benedict are successful.
Rainbird Valve modification of Marc Alan in CSSALT workgroup

2-Active PEEP sensor:
PEEP (Positive end-expiratory pressure): That is, at the end of exhalation , keeping the airway pressure slightly (5–10 cmH2O) above the atmospheric pressure, to prevent alveoli from collapsing completely, to facilitate re-inflation and to increase oxygen absorption. This PEEP pressure can be achieved by purely mechanical valves as well as by actively closing the exhalation valve early. The topic of the next chapter in this article is about my work on the active PEEP problem. The advantage of the active PEEP valve is that the pressure can be changed software-wise according to the patient’s condition.
3-Flow Sensor:
Venturi tube made of MPVX7002DP sensor and PVC solves the problem of flow sensor. You can find the flow sensor code of Bill Schmidt in the link below.
Flow sensor made of PVC pipe, emerging in CSSALT Working Group

Below is Bill Schmitt’s flow sensor code.
The Anti-Drowning Valve (made with a membrane that is partially adhered on the PVC Pipe) , high-pressure protection valve and mechanical PEEP valve made of 3D are other solutions in the group.
If we do not count the 3D printer parts, there are 2 things that I wouldn’t prefer but a bit late to intervene. The first one is the use of character LCD, and the other is the use of the BMP280 absolute pressure sensors instead of the differential pressure sensors.
In the next part of the article, I will talk about Active Peep I worked on.
Active PEEP Studies
In the working group, Gordon concentrates on the active peep problem and shares his work on a daily basis. There are deviations in the desired PEEP value and the actual PEEP value, and he is looking for volunteers to develop new methods. Meanwhile he is trying to solve the problem with Adaptive Finite Impulse Response Filter.
I think of the solution in 2007. A solution that can give the timing required to achieve desired PEEP pressure at the very first breath.
Initial Tests for Active PEEP Solution
Active peep application is not very popular, I proceed by confirming the results of each test I have done with the published articles I can reach.
An experiment I did with a 15 liter glass carboy: We can reach the desired 5cm-H2O PEEP pressure with a precision of 0.3cm-H2O after 2 measurements. With the algorithm similar to the tire inflation device I wrote years ago

Using the 15 liter glass carboy above and 8mm outlet hose (I am experimenting on a test lung with 10 ml / cm-H2O compliance and 5cm-H2O / liter / second resistance values.) I close and measure the valve above the PEEP pressure. Open Valve, Close Valve and Measure.. Open , Close , Measure .. And finally I can predict PEEP pressure in a single breath with an accuracy of 0.3cm-H2O.
Another alternative to estimate time for active PEEP pressure
In the group , it is asked if there is anyone to assist in calculating the RC time constant (resistance x compliance) of liver. I concentrate my research on the time coefficient which I find almost no resources except a graph.

All you have to do is solve the equation for “t” and convert it to microprocessor code.
t = RC.ln P / Po
Bingo. This is exactly the elapsed time when we measure the plateau pressure drops to 0.37 of its initial value.
Let me share the program code C here.

Unlike the first solution, in this solution, when the valve is closed, the static PEEP pressure can rise 5–10cm-H2O above the first calculated value. However, in 4–5 breaths, it converges to the desired value with adding-up the errors.
Gordon has other methods on active PEEP based on PID and controlling valve timing in a certain exhalation phase. All of them can be said to be successful. All that remains is the intensive testing and time.
According to group founder Gordon Gibby, the active PEEP related solutions in this group may be published in The American Society of Anesthesiologists. And two potential summary articles are being released with the goal of presenting them to the American Society of Anesthesiologists next fall.
FDA undergoes a two-stage review for the Emergency Authorization of the ventilator. After the design review, which was approved in April, it has to go through a series of intense tests that are in the second stage.
Gordon is giving the big news as of May 8.
Tens of tests are carried out for 6 different ventilator control strategies each for 30 sequential breaths and all of them are very successful. (PEEP pressure is 1cm-H2O accuracy and flow volumes deviate less than 10%.)
As of the last week of May, the control card, which is in a prototype state, is being revised and can be produced.
For now, we expect FDA approval after interactive reviews ,and after completing some responses awaited by the FDA ,regarding the manufacture of the parts.
“Even thinking about this” is extraordinary:
Perhaps, by making a contribution to one of the first FDA approved, intensive care unit standard emergency ventilator, you will get the reward of your efforts ,in the breath of a 72 year-old man. You did in the name of no-one, and even if your name is not mentioned in anywhere.
Breath In, Breath Out, Live
People sometimes think that everything has an end, that all their efforts are in vain … But sometimes — like these days that we realize how fragile and volatile life is- even it is a breath, in fact, no effort, nothing is in vain.
From the first breath we take to the last we breath give, while all of them are connected, and in a life where the sum of what we take is equal to the sum of what we give , does the end really matter ?
Aren’t we actually getting the results of all the things that we think we’re not. In the exact moment we think.
Finally, I would like to thank everyone who gave breath to this article and made it possible.
Başkan KALEZADE – Turkish Airlines